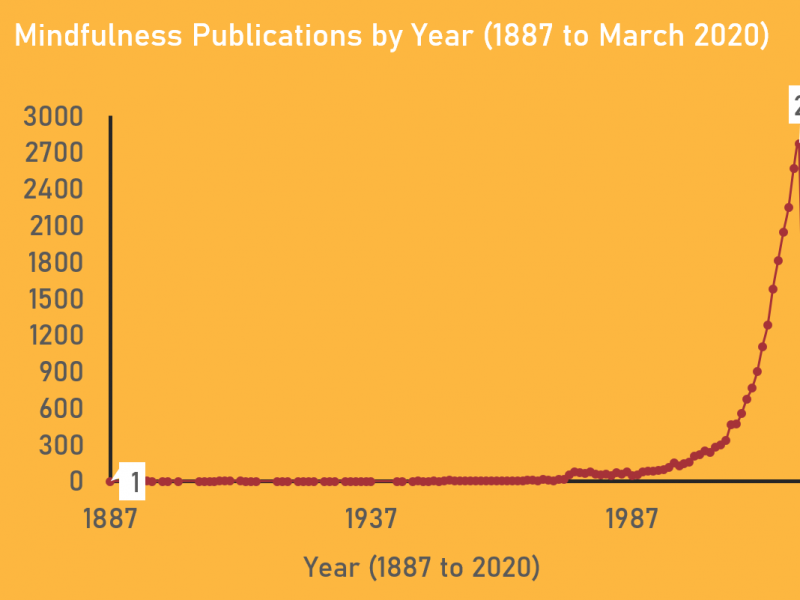
If you enter the keywords ‘mindfulness’ or ‘meditation’ in PubMed, a large database for biomedical research, you will retrieve over 20,000 references. This may come as no surprise for some, who have noticed that the term mindfulness is everywhere in the media. However, the investigation of secular mindfulness, which involves increasing moment-to-moment awareness of one’s bodily sensations, emotions and thoughts in a nonevaluative and accepting way, has not always been this popular in the Western world. If you look at Figure 1 below, which illustrates the results by year from the first publication in 1887 to March 2020, you will notice that the field only started to gain momentum in the 1990s. This coincides with the introduction of mindfulness-based programs (e.g. mindfulness-based cognitive therapy [MBCT]) to non-spiritual settings.[1]

As evidenced by the exponential rise in publications from the 1990s to 2019, we can see that the interest in mindfulness has surged greatly in a particularly short period of time. On the surface-level, this trajectory is quite exciting for the field of mindfulness research. However, what comes as a concern is that mindfulness-based programs (like MBCT) are now being applied in different populations (e.g. patients with anxiety and drug addiction) and contexts (e.g. corporations and prisons) although the evidence on the how, why, and for whom these programs work best is lagging far behind (Creswell, 2017). Mindfulness teachers and contemplative scientists argue that more research must be done with these questions at the forefront of the investigation before complex interventions such as MBCT are modified (Creswell, 2017; Alsubaie et al., 2017; van der Velden et al., 2015). With the application of mindfulness surpassing the evidence-base to support it, the aim of my DPhil is to develop a series of studies that will help dispel the myths of how, why, and for whom MBCT works best.
MBCT is a complex intervention with multiple components that can arguably have a salutary effect (Kuyken et al., 2010). Figure 2 below illustrates some of the core elements (e.g. individual MBCT practices, psychoeducational elements, the ‘group-effect’, and the ‘teacher-learner interaction effect’) that that make up the program. Numerous studies have demonstrated that MBCT can produce a range of benefits. Still, it is difficult to understand therapeutic change (in regards to what produces change, how and why change occurs, and for whom change occurs) when elements of MBCT are explored in combination rather than in isolation of each other. My DPhil thesis will address this by teasing apart the elements of MBCT and focus on the individual mindfulness practices as one core component.

Using quantitative and qualitative methods, as well as biometric assessments, I will explore the following questions: 1) Do MBCT practices produce change in the short-term and longer-term?; 2) What is the ‘dose-response’ relationship, in terms of how much practice is required to produce change in the short-term and longer-term?; 3) How, why, and for whom do these practices produce change?; and 4) Can individual accounts of these mindfulness experiences further our understanding of MBCT practices? The primary outcomes of interest include symptoms of depression and anxiety, and quality of life, in the general population.
The results from this thesis will create a platform to inform the general public on what secular mindfulness is and how it works. These findings will also be extremely useful for contemplative scientists, mindfulness teachers, and health-care professionals who are interested in developing bespoke mindfulness-based programs.
According to Figure 1, there were 2,773 mindfulness publications in 2019 alone and 650 studies have already been published in 2020, with the expectation that this number will surpass the 2019 numbers by the end of the year. Mindfulness research is now at a turning point and it is important that the evidence-base is prioritized and kept in the foreground.
Footnotes:
[1] MBCT is traditionally an eight-week course, comprised of weekly group sessions (1.5 to 2 hours in length), daily mindfulness practice (30 to 45 minutes per day), and other therapeutic components (see Figure 2). This program was developed by Mark Willams, John Teasdale and Zindel Segal to specifically treat patients with recurrent depression and studies have demonstrated therapeutic success (Williams & Kuyken, 2012; Piet, Würtzen & Zachariae, 2012).